

Grossing sample’s orientation in the cassette and during embedding follow up are the underestimated parts of grossing in surgical pathology. Although vast many of biopsy specimens do not require any orientation, actually it is impossible in some occasions, the orientation approach ought to be obligatory in grossing. In this regard, orientation of a tiny gastrointestinal or urinary bladder biopsy might sound unrealistic and unnecessary, but it is not right.
Every biopsy has an area of the most diagnostic value and the area of the specimen’s removal that can be seen by different color (in formalin fixed biopsy, it is a dot of formation of acid formalin hematin that makes blood tan brown). In the ideal world, the specimen ought to be oriented in the way that this area is laterally, not seen on the top and not concealed in the bottom). In this situation, all diagnostically valuable layers would be on the slide for the pathologist’s evaluation. If in a urinary bladder or gastric biopsy this might be seen as insignificant or in an esophageal biopsy impossible, such orientation of a duodenal biopsy would be very much desirable. In the case of a cervical biopsy it is definitely obligatory, otherwise the most diagnostically significant epithelial part, especially the area of transitional epithelium could be cut of or in the depth of the specimen below the microtome blade’s reach.
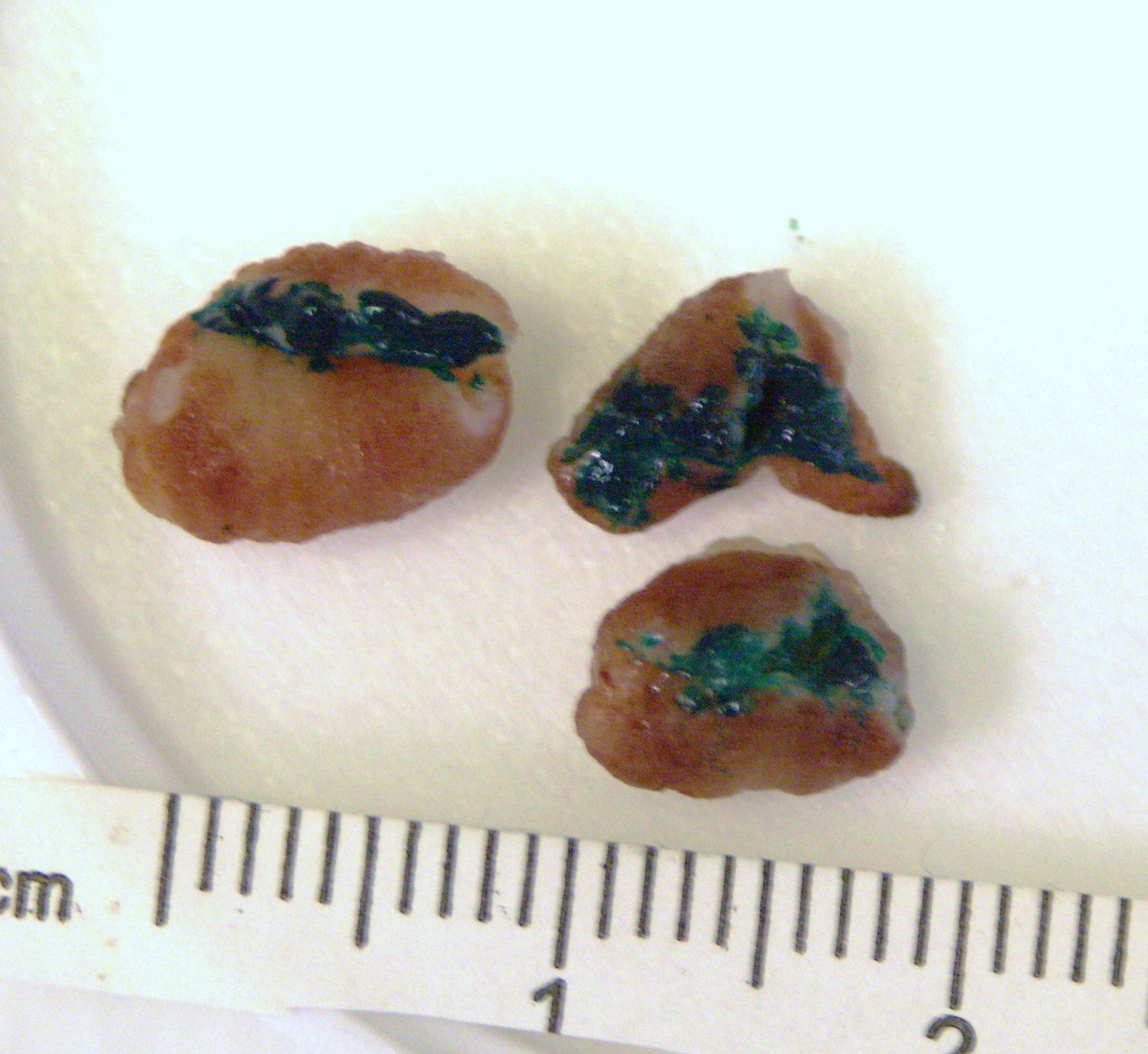

The biopsy area is inked
Prostate needle biopsy ideally also need an orientation, but it can be done only before fixation that is not achievable in USA practice when the specimen is received in prefilled formalin containers. But if the core were inked by the clinician immediately after obtaining the biopsy, this core can be processed with orientation. This procedure can have a significant diagnostic value. This is an example of biopsy orientation importance.
There are two main parts of the specimen orientation: before sampling in preparation to the specimen’s approach before the first cut and the sample’s orientation in the processing cassette. The first part reflects purely the specimen’s assessment from diagnostic point of view to bring the most diagnostically valuable areas to the pathologist’s attention. The second part includes technical consideration of embedding and microtomy.
From the technical point of view, effective specimen orientation requires immobilization of the area of interest before sampling. The “third hand principle”, the specimen immobilization against a vertical surface, allows the grossing person to approach the area of interest for a decisive, more or less uniform perpendicular cut. In a case of biopsy or diagnostically significant area (surgical margin, lesion), the suggested “adjustable immobilization” concept can play a role when the uniformity of the section is sacrificed for the sake of diagnostic value of the sample.
Ink and knife/blade do their part in presenting the most informative diagnostic sample. There are different techniques that can be used for proper orientation. While some techniques have fallen out of use and others remain in practice, techniques which have been forgotten are being brought back periodically, but with corrections.
There are many ways of specimen orientation in the processing cassette. Most of them are now abandoned as cumbersome and inefficient.
Embedding instructions
|
Marks |
Methods |
| Notes on the grossing log | Gelfoam with cyanoacrylate |
| Notes in or on cassettes | Agar-agar |
| Notches on the section | Cucumber slabs |
| Inking | Histo-Gel |
| What’s else? | Foam pads, others … |
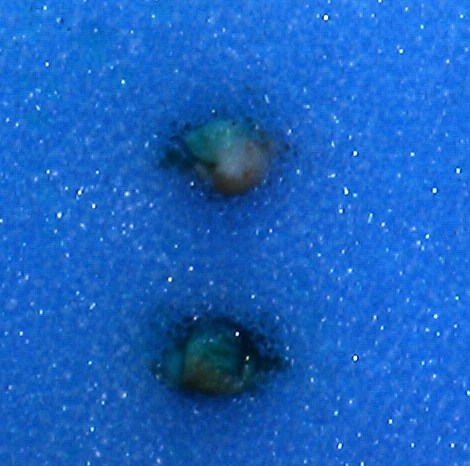
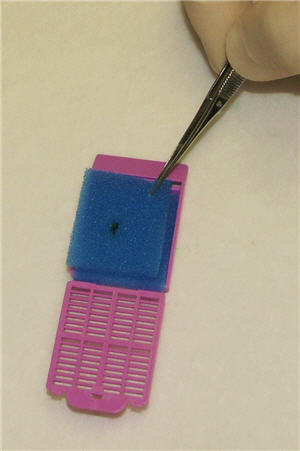
Two foam polyester pads used to sandwich the specimen in a position for embedding. This method is very popular, however this often does not help the embedding person to correctly orientate a biopsy, especially if it is too small or of uncertain shape. A rarely used method of superficial incisions in spongy pads was proposed for small biopsies. Complete incisions through the pad can make this method more universal, especially for orientation skin, cervical, and gastrointestinal polyps. This method is described in full in the article Biopsy Orientation in Surgical Pathology


Labia placed in the cassette with foam pad for the best orientation

The search for methods of specimen’s orientation continues. There are proposals of sectionable cassettes with fluoropolymer platforms or silicone pads for embedding orientation but they are still at the stage of testing.
The principle of sampling in the grossing room: eyes on specimen’s place in the embedding mold and under the microtom’s blade, in other words a histotechnologists’ set of mind. Correct orientation includes envision the trimming of the block, multiple slides, and possibilities that the microtomy ribbon is not always good requiring additional microsections.

Then starts the follow-up part of grossing technology. This website is relentlessly propagating this notion.